Hepatitis B
INFECTIOUS AGENT
Hepatitis B is caused by hepatitis B virus (HBV), a small, circular, partially double-stranded DNA virus in the Hepadnaviridae family.MODE OF TRANSMISSION
HBV is transmitted by activities that involve contact with blood, blood products, and other body fluids (such as semen). Such activities include the following:- Unprotected sexual contact
- Injection drug use with shared needles and injection paraphernalia
- Transfusions with blood or blood products that have not been screened for HBV
- Work in health care fields (medical, dental, laboratory) that entails exposure to human blood
- Dental, medical, or cosmetic (tattooing, body piercing) procedures with needles or other equipment that may be contaminated with blood
- Exposure to potentially contaminated blood through nonintact skin or mucous membranes
EPIDEMIOLOGY
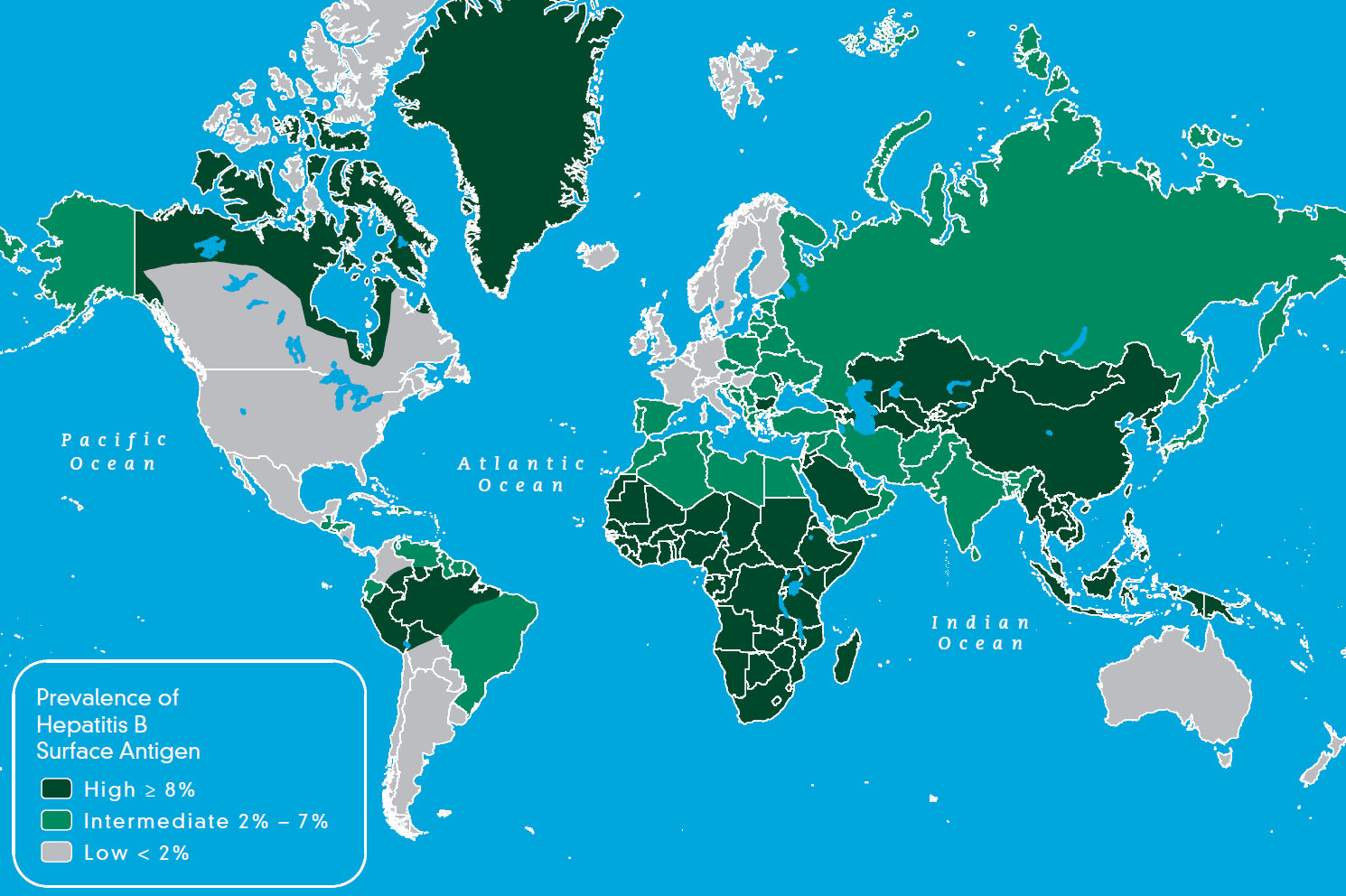
Map 3-04 shows the prevalence of chronic HBV infection globally. There are no data with which to assess the risk for HBV infection among US travelers. Published case reports of travelers acquiring hepatitis B during travel are rare. The risk for HBV infection among international travelers is low. However, the risk of HBV infection is considered higher in countries where the prevalence of chronic HBV infection is intermediate or high. Expatriates, missionaries, and long-term aid workers may be at increased risk for HBV infection.Map 3-04. Prevalence of chronic infection with hepatitis B virus, 2006


CLINICAL PRESENTATION
In adults and children aged ≥5 years, 30%–50% develop clinical illness typical of hepatitis B after initial exposure to the HBV. The incubation period for hepatitis B is 90 days (range, 60–150 days). Early symptoms that precede jaundice include constitutional symptoms like malaise, fatigue, and anorexia for about 1–2 weeks. The typical clinical signs and symptoms include nausea, vomiting, abdominal pain, and jaundice. In some cases, skin rashes, joint pain, and arthritis may occur. HBV infection is typically asymptomatic in children aged <5 years and immunocompromised adults. The overall case-fatality ratio of acute hepatitis B is approximately 1%.Acute hepatitis B progresses to chronic HBV infection in 30%–90% of people infected as infants or young children and in <5% of people infected during adolescence or adulthood. Chronic infection with HBV results in chronic liver disease, including liver cirrhosis and liver cancer.
DIAGNOSIS
Serologic markers, either alone or in combination, indicate different stages of HBV infection (Table 3-06). These serologic markers are typically used to differentiate between acute, resolving, and chronic infection.Table 3-06. Interpretation of serologic test results for hepatitis B virus infection
| SEROLOGIC MARKER | INTERPRETATION | |||
|---|---|---|---|---|
| HBsAg2 | TOTAL ANTI-HBc | IgM ANTI-HBc | ANTI-HbsAG | |
| – | – | – | – | Never infected |
| + | – | – | – | Early acute infection, transient (≤18 days) after vaccination |
| + | + | + | – | Acute infection |
| – | + | + | + or - | Acute resolving infection |
| – | + | – | + | Recovered from past infection and immune |
| + | + | – | – | Chronic infection |
| – | + | – | – | False-positive (susceptible), past infection, occult infection,3 or passive transfer of anti-HBc to infant born to HBsAg-positive mother |
| – | – | – | + | Immune if concentration is ≥10 mIU/mL after vaccine series completion, passive transfer after hepatitis B immune globulin administration |
Abbreviations: HBsAg, hepatitis B surface antigen; anti-HBc, antibody to hepatitis B core antigen.
1From: CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP). Part II: immunization of adults. MMWR Recomm Rep. 2006 Dec 8;55(RR-16):1–33.
2To ensure that an HBsAg-positive test result is not a false positive, samples with reactive HBsAg results should be tested with a licensed neutralizing confirmatory test, if recommended in the manufacturer’s package insert.
3Individuals positive only for anti-HBc are unlikely to be infectious except under unusual circumstances in which they are the source for direct percutaneous exposure of susceptible recipients to large quantities of virus (such as blood transfusion or organ transplant).
1From: CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP). Part II: immunization of adults. MMWR Recomm Rep. 2006 Dec 8;55(RR-16):1–33.
2To ensure that an HBsAg-positive test result is not a false positive, samples with reactive HBsAg results should be tested with a licensed neutralizing confirmatory test, if recommended in the manufacturer’s package insert.
3Individuals positive only for anti-HBc are unlikely to be infectious except under unusual circumstances in which they are the source for direct percutaneous exposure of susceptible recipients to large quantities of virus (such as blood transfusion or organ transplant).
TREATMENT
No specific treatment is available for acute hepatitis B. Antiretroviral drugs are approved to treat chronic hepatitis B.PREVENTIVE MEASURES FOR TRAVELERS
Vaccine
Indications for Use
Hepatitis B vaccination should be administered to all unvaccinated people traveling to areas with intermediate or high prevalence of chronic hepatitis B (hepatitis B surface antigen prevalence ≥2%). Hepatitis B vaccination is recommended for all US residents who work in health care settings that involve potential exposure to human blood. All unvaccinated children and adolescents (aged <19 years) should receive hepatitis B vaccine. Regardless of destination, all people who may engage in practices that place them at risk for HBV infection during travel (such as men who have sex with men, injection drug users, anyone who had a sexually transmitted disease or has had more than one sexual partner in the previous 6 months) should receive hepatitis B vaccination, if previously unvaccinated. Any adult seeking protection from HBV infection should be vaccinated; acknowledgment of a specific risk factor is not a requirement for vaccination.Vaccine Administration
The vaccine is usually administered as a 3-dose series on a 0-, 1-, 6-month schedule. The second dose should be given 1 month after the first dose; the third dose should be given ≥2 months after the second dose and ≥4 months after the first dose. Alternatively, the vaccine Engerix-B is approved for administration on a 4-dose schedule at 0, 1, 2, and 12 months. In addition, a 2-dose schedule for Recombivax HB has been licensed for children and adolescents aged 11–15 years. According to the 2-dose schedule, the second dose is given 4–6 months after the first dose. A 3-dose series that has been started with one brand of vaccine may be completed with another brand. Twinrix is a combined hepatitis A and hepatitis B vaccine licensed for people aged ≥18 years. Primary immunization consists of 3 doses, given at 0, 1, and 6 months.Special Situations
Ideally, vaccination should begin 6 months before travel so the full vaccine series can be completed before departure. Because some protection is provided by 1 or 2 doses, the vaccine series should be initiated, if indicated, even if it cannot be completed before departure. Optimal protection, however, is not conferred until after the final vaccine dose is received. Recently the Food and Drug Administration approved an accelerated vaccine schedule to be used for those traveling to endemic areas at short notice and facing imminent exposure or for emergency responders to disaster areas. An accelerated vaccination schedule with Twinrix (combined hepatitis A and hepatitis B vaccine) also can be used (doses at 0, 7, and 21–30 days). In this situation, a booster dose should be given at 12 months to promote long-term immunity. For children and adults with normal immune status who received the recommended vaccine series, pre-travel booster doses are not recommended (see Chapter 7, Vaccine Recommendations for Infants and Children). Serologic testing to assess antibody levels is not necessary for most fully vaccinated people.Vaccine Safety and Adverse Reactions
Hepatitis B vaccines have been shown to be safe for people of all ages. Pain at the injection site (3%–29%) and elevated temperatures >99.9°F (37.7°C) (1%–6%) are the most frequently reported side effects among vaccine recipients. These vaccines should not be administered to people with a history of hypersensitivity to any vaccine component, including yeast. The vaccine contains a recombinant protein (hepatitis B surface antigen) that is noninfectious.Limited data indicate no apparent risk of adverse events to the developing fetus when hepatitis B vaccine is administered to pregnant women. HBV infection in a pregnant woman can result in serious disease for the mother and chronic infection for the newborn. Neither pregnancy nor lactation should be considered a contraindication for vaccination.
Personal Protection Measures
As part of the pre-travel education process, all travelers should be given information about the risks for hepatitis B and other bloodborne pathogens from contaminated medical equipment, injection drug use, unprotected sexual activity, and other methods of transmission and be informed about prevention measures, including vaccination, to prevent transmission of HBV. When seeking medical or dental care, travelers should be alert to the use of medical, surgical, dental, and cosmetic (tattoo, piercing) equipment that has not been adequately sterilized or disinfected, reuse of contaminated equipment, and unsafe injecting practices (such as reuse of disposable needles and syringes). HBV and other bloodborne pathogens can be transmitted if tools are not sterile or if a tattoo artist or piercer does not follow proper infection control procedures. Travelers should consider the health risks when deciding to get a tattoo or body piercing in areas where adequate sterilization or disinfection procedures might not be available or practiced.BIBLIOGRAPHY
- Bock HL, Loscher T, Scheiermann N, Baumgarten R, Wiese M, Dutz W, et al. Accelerated schedule for hepatitis B immunization. J Travel Med. 1995 Dec 1;2(4):213–7.
- CDC. Updated US Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2001 Jun 29;50(RR-11):1–42.
- Lok AS, McMahon BJ. Chronic hepatitis B: update of recommendations. Hepatology. 2004 Mar;39(3):857–61.
- Long GE, Rickman LS. Infectious complications of tattoos. Clin Infect Dis. 1994 Apr;18(4):610–9.
- Mariano A, Mele A, Tosti ME, Parlato A, Gallo G, Ragni P, et al. Role of beauty treatment in the spread of parenterally transmitted hepatitis viruses in Italy. J Med Virol. 2004 Oct;74(2):216–20.
- Mast E, Goldstein S, Ward JL. Hepatitis B vaccine. In: Plotkin SA, Orenstein WA, editors. Vaccines. 5th ed. Philadelphia: WB Saunders; 2004. p. 199–337.
- Mast EE, Margolis HS, Fiore AE, Brink EW, Goldstein ST, Wang SA, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP). Part 1: immunization of infants, children, and adolescents. MMWR Recomm Rep. 2005 Dec 23;54 (RR-16):1–31.
- Mast EE, Weinbaum CM, Fiore AE, Alter MJ, Bell BP, Finelli L, et al. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP). Part 2: immunization of adults. MMWR Recomm Rep. 2006 Dec 8;55 (RR-16):1–33.
- Sagliocca L, Stroffolini T, Amoroso P, Manzillo G, Ferrigno L, Converti F, et al. Risk factors for acute hepatitis B: a case-control study. J Viral Hepat. 1997 Jan;4(1):63–6.
- Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M. Unsafe injections in the developing world and transmission of bloodborne pathogens: a review. Bull World Health Organ. 1999;77(10):789–800.

{kind=link}
{kind=link}