Hepatitis
C is caused by the hepatitis C virus (HCV), a spherical, enveloped,
positive-strand RNA virus, approximately 50 nm in diameter.
Transmission
of HCV is bloodborne and occurs mainly through sharing drug-injection
equipment, from transfusion of unscreened blood, or from untreated
clotting factors. In developing countries, unsterile medicinal and
other injection practices account for many infections. HCV is
infrequently transmitted through sexual contact.
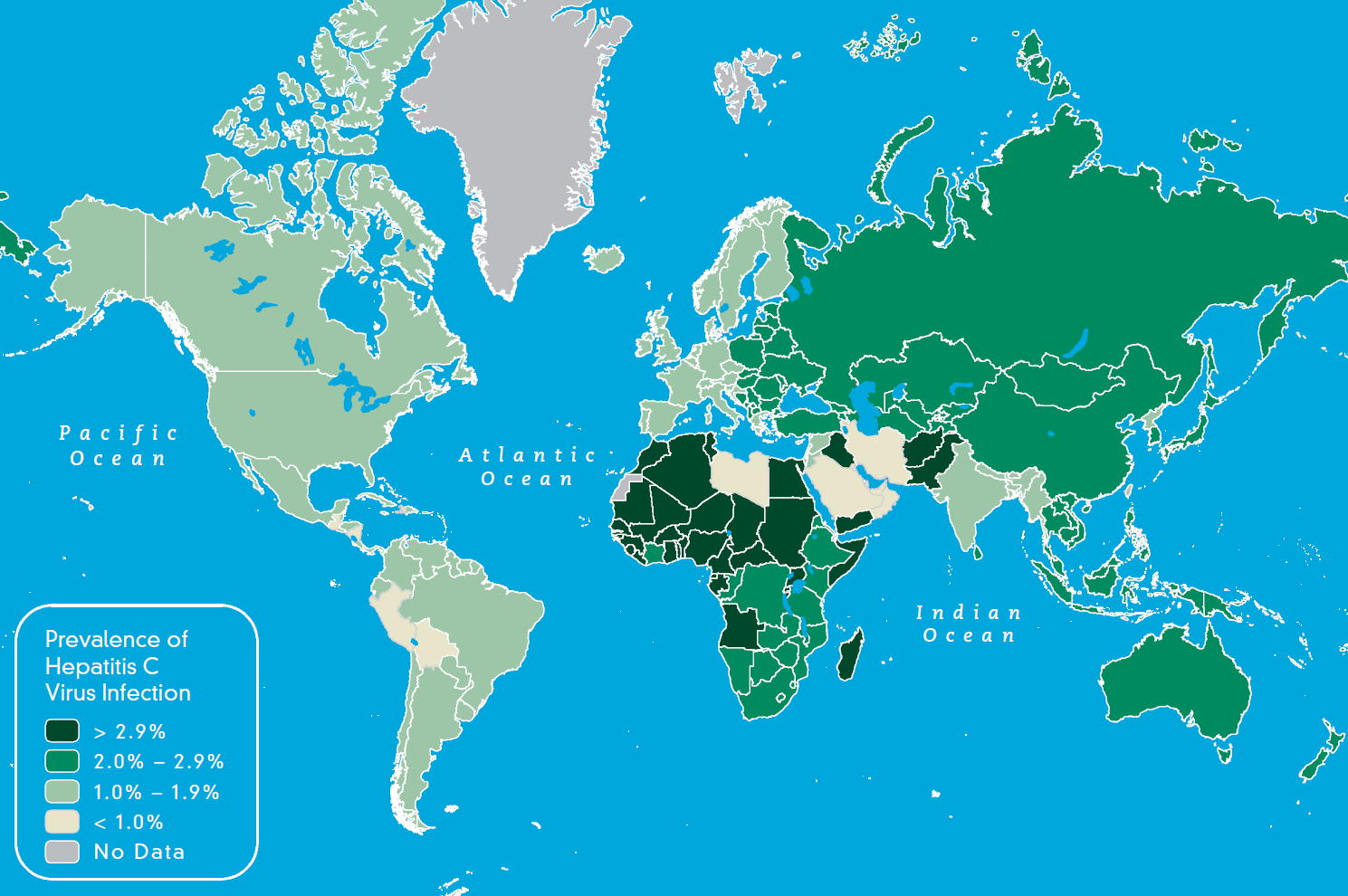
Approximately
3% (170 million) of the world’s population has been infected with HCV.
For most countries, the prevalence of HCV infection is <3%. The
prevalence is higher (up to 15%) in some countries in Africa and Asia
and highest (>15%) in Egypt (
Map 3-05).
The most frequent mode of transmission in the United States is through
sharing drug-injecting equipment among people who inject drugs.
Travelers’ risk for contracting HCV infection is generally low. For
international travelers, the principal activities that can result in
blood exposure are the following:
- Receiving blood transfusions that have not been screened for HCV
- Having medical or dental procedures
- Engaging in activities (such as acupuncture, tattooing, or
injecting drug use) in which equipment has not been adequately
sterilized or disinfected, or in which contaminated equipment is reused
- Working in health care fields (medical, dental, or laboratory) that entail direct exposure to human blood
Map 3-05. Prevalence of chronic hepatitis C infection

Most
people (80%) with acute HCV infection have no symptoms. If symptoms
occur, they may include loss of appetite, abdominal pain, fatigue,
nausea, dark urine, and jaundice. Approximately 75%–85% of HCV-infected
people develop chronic hepatitis C. The most common symptom of chronic
infection is fatigue; severe liver disease develops in 10%–20% of
infected people.
Two
major types of tests are available: IgG assays for anti-HCV and
nucleic acid amplification testing to detect HCV RNA in blood (viremia).
Assays for IgM, to detect early or acute infection, are not available.
Approximately 80% of people who seroconvert to anti-HCV, indicative of
acute infection, will progress to chronic infection and persistently
detectable viremia. False-negative antibody test results, while rare,
may occur early in the course of acute infection, usually in the first
15 weeks after exposure and infection.
Treatment
for hepatitis C is rapidly evolving. In general, “sustained viral
response” (considered a cure) is now achieved in 50% of patients taking
pegylated interferon and ribavirin for 24–48 weeks. New oral agents
added to a regimen of interferon and ribavirin are increasing cure
rates to 85%–90% on initial treatment attempts; these may be approved
and available by the time of printing this publication.
No
vaccine is available, and immune globulin does not provide protection.
When seeking medical or dental care, travelers should be alert to the
use of medical, surgical, and dental equipment that has not been
adequately sterilized or disinfected, reuse of contaminated equipment,
and unsafe injecting practices (such as reuse of disposable needles and
syringes). HCV and other bloodborne pathogens can be transmitted if
tools are not sterile or the clinician does not follow other proper
infection-control procedures (washing hands, using latex gloves, and
cleaning and disinfecting surfaces and instruments). There are still a
few areas of the world, such as parts of sub-Saharan Africa, where
blood donors may not be screened for HCV. Travelers should be advised
to consider the health risks if they are thinking about getting a
tattoo or body piercing in areas where adequate sterilization or
disinfection procedures might not be available or practiced.
- Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL,
Alter MJ. The prevalence of hepatitis C virus infection in the United
States, 1999 through 2002. Ann Intern Med. 2006 May 16;144(10):705–14.
- Global Burden Of Hepatitis C Working Group. Global burden of
disease (GBD) for hepatitis C. J Clin Pharmacol. 2004 Jan;44(1):20–9.
- Prati D. Transmission of hepatitis C virus by blood
transfusions and other medical procedures: a global review. J Hepatol.
2006 Oct;45(4):607–16.
- Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infect Dis. 2005 Sep;5(9):558–67.
- Shimakami T, Lanford RE, Lemon SM. Hepatitis C: recent
successes and continuing challenges in the development of improved
treatment modalities. Curr Opin Pharmacol. 2009 Oct;9(5):537–44.
- Simonsen L, Kane A, Lloyd J, Zaffran M, Kane M. Unsafe
injections in the developing world and transmission of bloodborne
pathogens: a review. Bull World Health Organ. 1999;77(10):789–800.
- Thompson ND, Perz JF, Moorman AC, Holmberg SD. Nonhospital
health care–associated hepatitis B and C virus transmission: United
States, 1998–2008. Ann Intern Med. 2009 Jan 6;150(1):33–9.

{kind=link}
Комментариев нет:
Отправить комментарий